
Graeme M. Clark
University of Melbourne

Ingeborg Hochmair
MED-EL

Blake S. Wilson
Duke University
The 2013 Lasker~DeBakey Clinical Medical Research Award honors three scientists who developed the modern cochlear implant, a device that restores hearing to individuals with profound deafness. Through their vision, persistence, and innovation, Graeme M. Clark (Emeritus, University of Melbourne), Ingeborg Hochmair (MED-EL, Innsbruck), and Blake S. Wilson (Duke University) created an apparatus that has transformed the lives of hundreds of thousands of people. Their work has, for the first time, substantially restored a human sense with a medical intervention.
When hearing fades, so does part of the world. People miss out on conversations, their toddler’s footsteps, and cars screeching around corners. Childhood deafness impairs the ability to understand spoken language and acquire speech, and these hindrances limit educational trajectories and career choices. Cochlear implants return the capacity to communicate and connect through one of the primary conduits used by the vast majority of humans.
Whispers of a solution
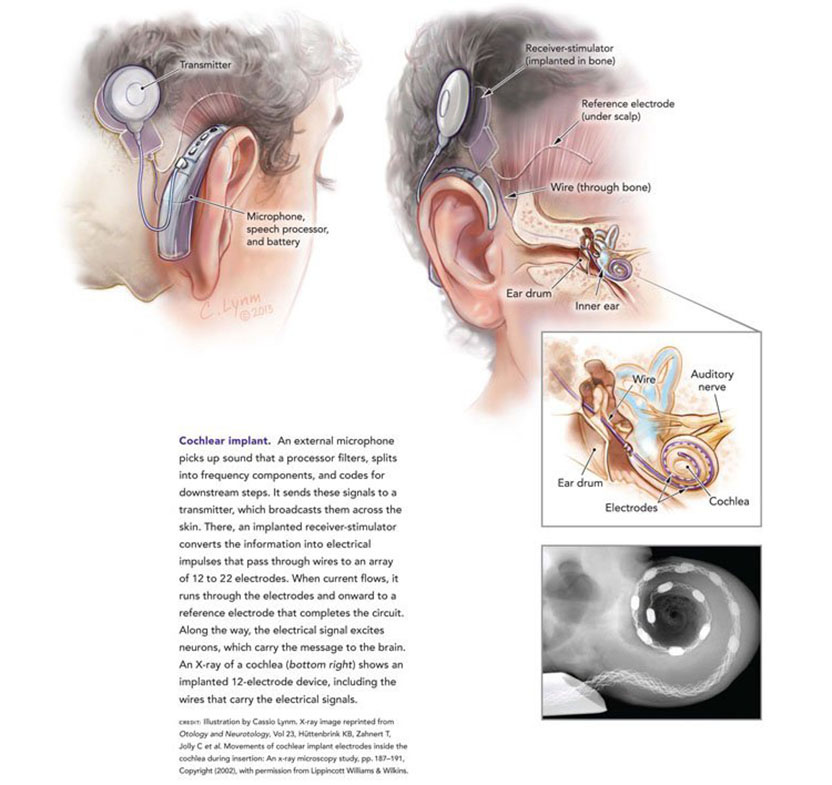
In normal hearing, auditory structures capture sound and translate it into information that the brain can interpret. The ear canal funnels vibrations onto the eardrum, and movements there perturb tiny bones, which propagate the fluctuations to the inner ear. Waves roll through the fluid-filled cochlea, a snail-shaped tube, and bend the thousands of delicate hair cells that lie within this organ. The displacements cause the hair cells to produce an electrical signal that stimulates the eighth cranial nerve — sometimes called the auditory nerve — and the message continues to the brain.
Within that chain of events, numerous things can go wrong. In most cases, severe hearing loss arises from damage to or absence of the sensory hair cells. Cochlear implants bypass the need for these cells by using electrical stimuli to directly excite the auditory nerve.
In the late 1950s, French doctors made a rudimentary effort to implement this idea in an individual whose hearing gear was largely gone. The system worked poorly and failed quickly, but news of the attempt reached and inspired the late otologist William House in California. He dreamed of designing a robust, easily usable prosthesis that would help deaf people hear for their lifetimes.
House developed an apparatus that delivered current through a single wire, or electrode, to a single spot on the cochlea. In 1961, two individuals received this implant. It enabled them to perceive environmental sounds, and its descendant devices helped people read lips, but speech was extremely distorted. Nevertheless, this triumph kicked off a bustle of activity among a few scientists who aimed to improve the device.
Most experts, however, did not join these pioneers, but instead cast skepticism on the enterprise. Restoration of meaningful hearing was impossible with electrical stimulation, they decried. The required neural response was far too complicated to replicate by simple and coarse signals.
Channels to hearing
Fortunately, Ingeborg Hochmair and Graeme Clark did not shy away from daunting challenges. Independently, they set out to craft an apparatus that would not only enhance awareness of the surroundings and facilitate lip reading, but would also enable deaf people to comprehend speech without visual cues. To do so, the investigators exploited a part of the auditory network that the single-electrode approach ignored.
In a person with intact cochlear hair cells, these structures beat every time sound waves hit. The perturbations cause neurons to fire in synch with the pulses, and single-electrode tactics rely on this ‘time coding’ system (so named because its operation depends on how often vibrations arrive). By the end of the 1960s, studies by the late Blair Simmons (Stanford University) suggested that single electrodes could reliably convey tones only up to a certain frequency. Above that point, further increases did not register as higher pitches to most people.
Simmons proposed that the time code alone would not allow faithful auditory perception; a second strategy that our brains use to decipher sound was needed in addition. The hair cells along the cochlea do not react uniformly to a given incoming pitch; their locations matter. A baby’s cry awakens hair cells — and thus, the nerves they excite — at the cochlea’s opening, whereas a rumbling truck disturbs those in the spiral’s center. As a result, the unfurled cochlea bears similarities to a piano, with pitch proceeding in an orderly fashion from highest to lowest. Together, the ‘notes’ in different places communicate all tones to the brain.
Clark and Hochmair — with electrical engineer (and future husband) Erwin Hochmair — harnessed this ‘place coding’ phenomenon by routing particular speech sounds to different parts of the cochlea. In this way, they selectively targeted nerves that respond especially well to the frequencies received. The scientists deployed multiple electrodes, each of which resided at a different site on the cochlea’s inner surface.
In addition to solving the electrical challenges, they and others in the field also tackled numerous safety and mechanical issues. For example, the devices — and the techniques for implanting them — needed to minimize infection risk, tissue damage, and hazards associated with running current through a person’s body. The investigators had to find nontoxic materials that were inert to biological activities and formulate ways to thread electrode arrays deep into the cochlea and position them there.
Each of their designs includes components that, together, transform acoustical information into electrical signals that excite the auditory nerve (see Figure).
Patients were first implanted with the Hochmair and Clark inventions in December 1977 and August 1978, respectively. These multichannel prototypes dramatically upgraded speech perception. Many of today’s systems mirror the basic blueprint of the original devices.
In 1985, the US Food and Drug Administration gave its inaugural approval to a multichannel cochlear implant— for treating adults who could hear before they went deaf. Three years later, an NIH consensus statement concluded that multichannel stimulation would probably produce superior speech recognition than single-channel stimulation.
Breaking sound barriers
Although the early-generation multichannel devices had propelled implants to a new performance level, many recipients could not grasp spoken words or sentences without contextual or visual hints. The next major development catapulted the technology over this hurdle.
In 1991, Blake Wilson reported a new speech-processing strategy that provides time- and place-coding information in a particularly clear way. It rapidly presents a wide range of frequency pulses that are slightly offset in time from one another, or ‘interleaved’. Because no two electrodes receive a signal simultaneously, the scheme minimizes distortions and omissions. Through this and other important features, Wilson’s ‘continuous interleaved sampling’ (CIS) system has allowed the majority of cochlear implant recipients — for the first time — to understand words and sentences with no visual cues. CIS supplies the basis for the sound-processing strategies that are now widespread and fueled an exponential growth in implant use that began in the early 1990s. Its rapid introduction, utilization, and dissemination stemmed in large part from a policy that donates to the public domain all intellectual property produced by Wilson and his colleagues from their NIH-funded cochlear-implant research.
Today, most people with cochlear implants can talk on their cell phones and follow conversations in relatively quiet environments. Experts complain that patients are doing so well, they’re hitting ceilings on standard hearing tests, which lack the sensitivity to demonstrate the subtle deficits in speech comprehension that a typical recipient experiences. Additional advances are moving the field toward the ability to fine-tune hearing and thus help people fully appreciate music and understand tone languages, which are spoken by a large fraction of the planet’s population.
Amplifying improvements
As of 2010, approximately 219,000 people across the globe had received cochlear implants, and more than 80% of the prostheses had been dispensed since 2000. The numbers are increasing rapidly; by the middle of 2013, more than 320,000 individuals were using cochlear implants, and almost 40,000 had one in each ear.
As the device’s effectiveness has grown, so too has the number of potential candidates. Now, adults who have severe age-related hearing loss, for instance, are taking advantage of the invention.
Cochlear implants have delivered exceptionally dramatic effects to children. If a person can’t hear during the first few years of life, the brain can’t fully equip itself to understand and acquire speech. Early intervention is therefore crucial. Of every 1000 babies born, more than one is deaf.
Today, about 60% of implants worldwide go to children; those who live in an industrialized nation routinely receive them between age 1 and 2 years. With this intervention, many youngsters can more easily mainstream into regular schools.
Some individuals now receive implants in both ears, which is especially helpful not only to enrich hearing in general, but also for localizing speech in noisy settings. People are also combining cochlear implants with hearing aids to get the most out of both instruments; for example, electrical stimulation in the areas of the cochlea that respond to high frequencies can synergize well with hearing aids that enhance low-frequency perception.
Brilliance and relentless commitment have fueled the reverberating success of Clark, Hochmair, and Wilson. Less than a generation ago, deaf individuals had no hope of hearing again. These scientists have cracked the barriers that formerly isolated huge numbers of people from the realm of sound and have made many lives hum in new ways.
by Evelyn Strauss
Key publications of Graeme M. Clark
Clark, G.M., Pyman, B.C., and Bailey, Q.R. (1979). The surgery for multiple-electrode cochlear implantations. J. Laryngol. Otol. 93, 215-223.
Clark, G.M., Blamey, P.J., Brown, A.M., Gusby, P.A., Dowell, R.C., Franz, B.K.-H., Pyman, B.C., Shepherd, R.K., Tong, Y.C., Webb, R.L., Hirshorn, M.S., Kuzma, J., Mecklenburg, D.J., Money, D.K., Patrick, J.F., and Seligman, P.M. (1987). The University of Melbourne — Nucleus multi-electrode cochlear implant. Adv. Otorhinolaryngol. 38, 1-181.
Busby, P.A., Whitford, L.A., Blamey, P.J., Richardson, L.M., and Clark, G.M. (1994). Pitch perception for different modes of stimulation using the cochlear multiple-electrode prosthesis. J. Acoust. Soc. Am. 95, 2653-2669.
Key publications of Ingeborg Hochmair
Hochmair-Desoyer, I.J., Hochmair, E.S., Rischer, R.E., and Burian, K. (1980). Cochlear prostheses in use: Recent speech comprehension results. Arch. Otorhinolaryngol. 229, 81-98.
Hochmair-Desoyer, I.J., Hochmair, E.S., Burian, K., and Fischer, R.E. (1981). Four years of experience with cochlear prostheses. Med. Prog. Technol. 8, 107-119.
Hochmair-Desoyer, I.J., Hochmair, E.S., Burian, K., and Stiglbrunner, H.K. (1983). Percepts from the Vienna cochlear prosthesis. Ann. N. Y. Acad. Sci. 405, 295-306.
Key publications of Blake S. Wilson
Wilson, B.S., Finley, C.C., Lawson, D.T., Wolford, R.D., Eddington, D.K., and Rabinowitz, W.M. (1991). Better speech recognition with cochlear implants. Nature. 352, 236-238.
Wilson, B.S., Finley, C.C., Lawson, D.T., Wolford, R.D., and Zerbi, M. (1993). Design and evaluation of a continuous interleaved sampling (CIS) processing strategy for multichannel cochlear implants. J. Rehabil. Res. Dev. 30, 110-116.
Wilson, B.S. and Dorman, M.F. (2008). Cochlear implants: A remarkable past and a brilliant future. Hear. Res. 242, 3-21.
Award presentation by Jeremy Nathans
 In the New Testament, we read in the Gospel of Mark that Jesus performed the miracle of restoring hearing to a deaf man. Two thousand years later, modern medical science has developed a device that can deliver the same miraculous result, although, I should note, not with the same rapidity as the procedure described in the Gospel. That device is the cochlear implant, which functions as an electronic ear, converting sounds, such as speech, into tiny electrical impulses that activate the auditory nerve.
In the New Testament, we read in the Gospel of Mark that Jesus performed the miracle of restoring hearing to a deaf man. Two thousand years later, modern medical science has developed a device that can deliver the same miraculous result, although, I should note, not with the same rapidity as the procedure described in the Gospel. That device is the cochlear implant, which functions as an electronic ear, converting sounds, such as speech, into tiny electrical impulses that activate the auditory nerve.
Today we honor three pioneers — Graeme Clark, Ingeborg Hochmair, and Blake Wilson — who have devoted their professional lives to making the cochlear implant a reality. Their work, together with the work of many hundreds of engineers, audiologists, and surgeons, has brought the gift of hearing to several hundred thousand profoundly hearing-impaired individuals, a number that is climbing rapidly.
Acceptance remarks

Acceptance remarks, 2013 Lasker Awards Ceremony
I feel very honored to be a co-recipient of the prestigious Lasker~DeBakey Award in Clinical Medical Research, especially as it recognizes research that has led to the multi-channel cochlear implant or bionic ear — the first clinically successful interface between the world and human consciousness. It is also the first advance in helping severely-to-profoundly deaf children communicate since Sign Language of the Deaf began 250 years ago.
My passion to help deaf people started as a teenager when I experienced what it was like for my deaf father as a pharmacist in country Australia — he said years later of his deafness “it has been an enormous handicap, it affects your whole life, there is nothing so embarrassing as not being able to hear people properly.” But in 1967, when I started my research journey there was much skepticism — it had been said “direct stimulation of the auditory nerve fibres with resultant perception of speech is not feasible.”
Nevertheless, I commenced an uncertain journey by leaving a senior surgical position to do research in auditory brain science. And when I discovered in 1970 that multi-channel electrical stimulation would be needed there was nowhere to go to further the research. Fortunately, the University of Melbourne appointed me to establish the first ENT and audiology departments in Australia, but I still had few staff and little money. I pay tribute to the young graduates who shared the vision, stood on the streets of Melbourne shaking a tin and asking for money, and turned the ENT Department into an engineering one.
When all was ready, I interviewed my first experimental patient, Rod Saunders, in 1978. He said: “I would like to be able to hear something again. It’s a nightmare being deaf. If it helps with speech I will be very grateful.” It has also been a means of learning about brain function and what underlies human consciousness. I can now say after a tumultuous ride personally, that Rod and many thousands like him can now have their life back again. This has been in no small measure due to an exciting partnership with Cochlear and their leadership in biomedical technology.
In conclusion, I would to thank the Lasker Foundation again for this honor, and I will endeavor to continue my search for excellence to help deaf people and others with neurosensory disorders such as blindness and paraplegia.

Acceptance remarks, 2013 Lasker Awards Ceremony
The cochlear implant is not a life-saving device. It is, however, very, very special, since it has to do with communication, with being able to take part in society. It is connected with every child’s human right for education, and it can alleviate isolation and cognitive decline in older adults.
Clinical medical research is of particular importance in the field of CIs for at least three reasons:
Efficacy with CIs has to do with how well the sensory organ is replaced, it has to do with perception.
Secondly, since learning is involved with electrical stimulation, immediate and acute results of sound perception tests do not necessarily represent what the user will be able to perceive after getting used to the new input to their auditory system.
And thirdly, another very special aspect of cochlear implants is the enormous responsibility researchers and developers have to gently preserve the tiny delicate structures of the inner ear for future technologies. This is of special relevance with children born today with a life expectancy of maybe 120 years and with candidates who nowadays typically have hearing still present, that they hope and expect to be preserved.
Acceptance remarks, 2013 Lasker Awards Ceremony
Development of the modern cochlear implant was a worldwide effort involving many scientists, engineers, physician-scientists, and research subjects. The success of this effort is an outstanding example of the power of collaborations between the public and private sectors and also the informed support by the NIH of applied as well as basic research.
I am proud to stand before you today as a representative of the worldwide effort, and I am especially proud to stand with Graeme Clark and Ingeborg Hochmair, who are two of my heroes and the foremost living pioneers in our field.
Although the present cochlear implants are truly wonderful, room still exists for improvements. A variability in outcomes remains, and even the top-performing patients experience difficulties in understanding speech in adverse acoustic environments such as noisy restaurants or workplaces. In addition, reception of sounds more complex than speech — such as music — is less than satisfying for most patients. Research is underway to narrow or even eliminate these gaps between prosthetic and fully functional hearing, and to narrow the range of outcomes such that all patients will achieve high levels of performance. Many promising possibilities are being pursued by extraordinarily talented investigators, and I am completely confident that further improvements will be made.
An even more important challenge — in my mind — is to make the highly effective technology we have today available to all persons who could benefit from it. Thus far, about 320 thousand persons have received a cochlear implant in one or both ears. But various estimates indicate that as many as 25 million persons worldwide could benefit from a cochlear implant. That means that only about 1 or 2 percent of the population who could benefit actually have received a cochlear implant.
The cochlear implant is a transformative technology that allows children to be mainstreamed into regular schools, adults to have a wide range of job opportunities, and all recipients to connect in new and important ways with their families, friends, and society at large. The resulting human and economic benefits are immense.
In many parts of the world, cost is a barrier to widespread applications of the technology, even though the benefits ultimately far outweigh the cost. The principal expenses are in providing the appropriate medical infrastructure and care. The cost of the device also plays a role, but that cost is coming down and is not the dominant factor for most countries. Several of us in this room are working to reduce or remove the cost barrier, and to improve hearing health care worldwide, which includes prevention, screening, and treatments in addition to cochlear implants.
This magnificent award will greatly increase awareness of how cochlear implants can enable severely and profoundly deaf persons to realize their full potential in life, and that awareness will in turn facilitate further dissemination and development of this marvelous technology. Thank you for welcoming Graeme, Ingeborg, and me into the Lasker family, and thank you for the highly favorable tailwind you have given us and our colleagues to do more!
Interview with Graeme M. Clark, Ingeborg Hochmair, and Blake S. Wilson
Video Credit: Susan Hadary
