
Joel Habener
Massachusetts General Hospital

Lotte Bjerre Knudsen
Novo Nordisk

Svetlana Mojsov
The Rockefeller University
For the discovery and development of GLP-1-based drugs that have revolutionized the treatment of obesity
The 2024 Lasker~DeBakey Clinical Medical Research Award honors three scientists for their discovery and development of GLP-1-based drugs that have revolutionized the treatment of obesity. Joel Habener (Massachusetts General Hospital) and Svetlana Mojsov (The Rockefeller University) discerned the physiologically active form of the hormone, and Lotte Bjerre Knudsen (Novo Nordisk) turned it into medications that promote weight loss.
Globally, almost 900 million adults are living with obesity. In the United States, it afflicts as many as 40% of adults; in Europe the prevalence approaches 25%. The excess pounds underlie multiple life-threatening conditions. Obesity is commonly viewed as a failure of willpower, yet for many, diet and exercise don’t cure the problem. Historically, attempts to make safe and effective drugs that help people slim down have fallen short. Habener, Mojsov, and Knudsen have introduced a new era of weight management in which GLP-1-based pharmaceuticals promise to dramatically enhance health.
Hooking a new hormone
In the mid-1970s, Habener, a newly minted endocrinologist, set up his lab at Massachusetts General Hospital, and diabetes soon caught his attention. Normally, glucose goads the pancreas to release insulin, which ushers the sugar out of the bloodstream and into cells. In diabetes, a dearth of insulin keeps blood glucose levels high while cells starve. Although supplying insulin underpinned one form of therapy, researchers were exploring alternative tactics. Another pancreatic hormone, glucagon, boosts blood sugar concentrations, so thwarting it might benefit people with diabetes, the thinking went.
Habener decided to utilize the new tools of molecular biology and isolate the gene that encodes glucagon. NIH guidelines on recombinant DNA research at the time restricted manipulation of mammalian genes, so he pivoted to the anglerfish, which offered an advantage, as it contains a special organ that manufactures generous amounts of glucagon.
Scientists knew that active peptide hormones are liberated from larger proteins by enzymes that snip in specific places. In 1982, Habener reported that the fish glucagon gene encodes a predicted precursor protein that contains glucagon and, in addition, a second peptide that resembles glucagon. The same pair of amino acids, lysine-arginine, that mark cleavage sites in other hormone precursor proteins appears at several spots. Cutting there would free glucagon and the second peptide.
The following year, Graeme Bell (Chiron Corporation) found that the hamster glucagon-encoding gene also encodes a version of the second fish peptide, which he called glucagon-like peptide-1 (GLP-1). Similar results from human and other mammals followed.
An overlooked processing step?
By this time, chemist Svetlana Mojsov at The Rockefeller University had independently become a glucagon aficionado. She wanted to devise a way to produce large quantities of it for mechanistic studies. As part of this effort, she had pored over the hormone’s structure as a graduate student, postdoctoral fellow, and researcher. Mojsov’s thesis advisor, Bruce Merrifield (1969 Albert Lasker Basic Medical Research Award; 1984 Nobel Prize in Chemistry), had invented so-called solid phase protein synthesis, and by the mid-1970s, it had become the technique of choice for rapidly producing ample supplies of clean material.
Unfortunately, due to glucagon’s chemical peculiarities, certain amino acids undergo side reactions with the strong acid that the process requires. For this reason, conventional wisdom held that glucagon did not lend itself to the solid phase method.
This hurdle did not deter Mojsov. She conceived an alternative strategy that avoided strong acids. Furthermore, her approach produced a degree of purity never before achieved for peptide synthesis. The high yields and absence of contaminants would prove crucial for numerous aspects of her future work.
By 1983, when Mojsov moved to Massachusetts General Hospital as director of its peptide synthesis facility, she had improved the scheme and had begun to apply her expertise to GLP-1. The peptide intrigued her in part because she thought that it might fill a longstanding gap. In the early 1900s, scientists proposed that substances in the gut spur the pancreas to churn out hormones. Solid evidence for such “incretins” emerged in 1964, when researchers demonstrated that ingested glucose elicits more insulin release than injected glucose does. Something in the intestine, they concluded, provokes insulin secretion. Such incretins had thus far eluded identification and GLP-1, a previously unknown peptide that resembles a hormone (glucagon) known to influence blood-sugar levels, shined as a candidate.
Mojsov puzzled over the predicted sequence of GLP-1’s supposed 37-amino-acid chain. The presence of the same amino acids in the same positions of different proteins suggests that they perform an important function, yet GLP-1 begins with a stretch of six amino acids that don’t exist in glucagon or other molecular relatives. Mojsov eyed an arginine at position 6. Arginines are clipped by well-known human enzymes, and if GLP-1 started after that amino acid, the resulting peptide—now 31 rather than 37 amino acids in length—would align perfectly with its glucagon family members.
Getting to the crux of the GLP-1 matter
Mojsov set out to determine whether the shorter version of GLP-1[GLP-1 (7-37)] might be liberated from the longer one [GLP-1 (1-37)] and serve as the missing incretin. Toward that end, she synthesized large amounts of each pure peptide in single batches, thus setting herself up to ensure consistency in subsequent studies. She made antibodies that bind a common region; therefore, they recognize both variants. Crucially, she also figured out how to segregate GLP-1 (1-37) and GLP-1 (7-37) from within a mixture, exploiting the charge on the amino acids that are unique to the longer molecule. These innovations equipped her to find GLP-1 in tissue, distinguish GLP-1 (7-37) from GLP-1 (1-37), and pinpoint the active peptide.
Thus, the pièces de résistance in the early stages of the GLP-1 discoveries were these invaluable reagents and methods, which provided scientists with the means to draw unambiguous conclusions about essential aspects of GLP-1 biology.
Mojsov then conducted the first set of definitive experiments. She radioactively tagged her peptides and deployed them with GLP-1 antibodies to check whether GLP-1 shows up in animals. It does. Mojsov then separated the peptides and established that the truncated GLP-1 (7-37) composes a significant fraction of the total. This smaller peptide thus exists in nature and, notably, in the intestine, Mojsov, Habener, and their collaborators reported in 1986.
Mojsov and Habener teamed up with Gordon Weir (Joslin Diabetes Center) and, in 1987, demonstrated that tiny concentrations of pure GLP-1 (7-37), such as those in the bloodstream, stimulate insulin secretion from isolated rat pancreases that continue to function even when removed from the body. The longer form remains inert even at 10,000-fold higher concentrations. These observations revealed that GLP-1 (7-37), hereafter referred to as GLP-1, is the physiologically relevant peptide.
Habener and Mojsov then advanced to human studies. With David Nathan (Massachusetts General Hospital), they determined that GLP-1 prompts insulin release and lowers circulating blood glucose levels. This 1992 publication built the case that the hormone might provide the foundation for a safe diabetes drug, and several companies, including Novo Nordisk, AstraZeneca, Eli Lilly, and GSK latched onto this idea. Soon GLP-1’s potential would expand.
Fatty acids, plump with potential
A couple of years later, Knudsen took the helm of GLP-1 therapeutic development at Novo Nordisk, and in 1996, a paper caught her attention. Stephen Bloom (Hammersmith Hospital, London) had injected GLP-1 into rats’ brains, and the animals’ food intake plummeted. The peptide, Bloom proposed, sends a satiety signal.
The possibility that the hormone might fight obesity as well as diabetes had already piqued Knudsen’s interest due to hints from earlier animal studies led by Ole Madsen (Hagedorn Research Institute, Copenhagen). The notion that a molecule pegged for one disease could also combat another broke convention, and as Knudsen championed the idea, she faced resistance. To harness it for either use, though, she had to overcome a show-stopping limitation.
In the human body, GLP-1 vanishes minutes after it enters the bloodstream. An enzyme called dipeptidyl peptidase 4 (DPP-4) chews it up and the kidneys purge the rest. To transform GLP-1 into a drug, scientists would need to render it able to survive these assaults. Knudsen aimed to make an agent that would remain active for 24 hours after a single injection under the skin.
After toying with a slow-release formulation and ones that resisted DPP-4-mediated destruction, she settled on a strategy of attaching fatty acids to GLP-1. Fatty acids naturally adhere to an abundant protein in the circulation called albumin, which transports substances around the body. According to Knudsen’s vision, albumin would ferry its GLP-1 cargo through the bloodstream while protecting it from enzymatic destruction and renal filtration. The fatty acid would gradually unleash GLP-1 so that it can grasp its receptor on target cells and trigger its effects.
Knudsen’s team made GLP-1 analogs that varied in several ways, including fatty-acid length and type, attachment site within GLP-1, and chemical linker. Then the investigators assessed the compounds’ behavior. They aimed to stabilize the peptide and lengthen its longevity in animals while maximizing potency and keeping the amino acid sequence as close as possible to that of human GLP-1 to circumvent immunoreactivity. Two papers, in 2000 and 2007, detailed the results.
The researchers zeroed in on a candidate that they named liraglutide (see Figure). They had extended its half-life after subcutaneous injection from 1.2 to 13 hours. It performed well in a 2010 clinical trial of 1300 people with type 2 diabetes, and adverse events were mostly mild or moderate. The European Medicines Agency (EMA) approved liraglutide (Victoza®) to control blood sugar levels in type 2 diabetes in 2009, and the U.S. Food and Drug Administration (FDA) followed the next year. Liraglutide thus became the first once-daily GLP-1-based drug.
A feast of success
In the meantime, accumulating data supported the notion that GLP-1 reduces appetite and body weight, and Knudsen’s team pursued liraglutide for this purpose. In a key study, nondiabetic, obese or overweight subjects lost an average of more than 12 pounds over a year. More than one-third of the individuals in the liraglutide group lost at least 5% of their body weight and almost one-fourth lost more than 10%. Liraglutide makes people feel more satiated and less hungry, so they voluntarily eat less. The FDA and EMA gave it the green light in 2014 and 2015, respectively, and it was the first GLP-1-based drug approved for the treatment of obesity (Saxenda®).
The Novo Nordisk scientists wanted to go a step further; make the medicine last not for a day, but for a week. It would have to stick optimally to albumin: tightly enough to persist longer in the body, but loosely enough that sufficient quantities would let go to bind the receptor.
The team that sought this therapeutic, led by chemists Jesper Lau and Thomas Kruse, replaced one amino acid in GLP-1 with a molecule that confers resistance to DPP-4 cleavage and then systematically tested different fatty acids and chemical linker combinations. The investigators combed through about 4000 compounds to home in on one whose half-life grew dramatically—to 165 hours. They named it semaglutide (see Figure).
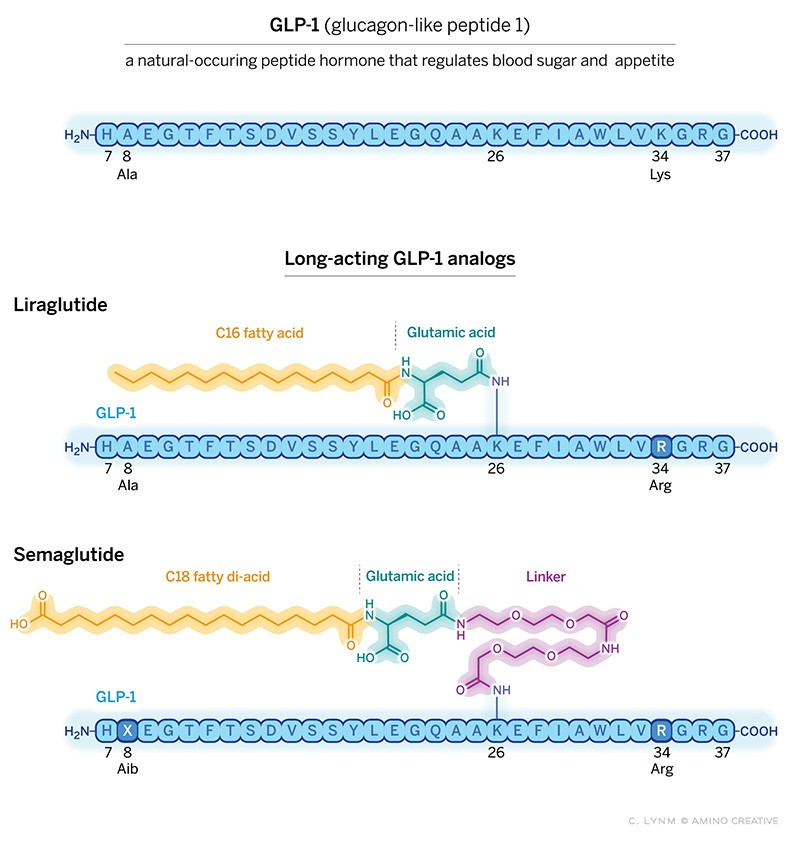
Weighty medicines
GLP-1 (top) serves as the active agent in two long-acting drugs, liraglutide (middle) and semaglutide (bottom), that offer new hope to people who are obese or overweight. These pharmaceuticals rely on fatty acid attachments to bind the bloodborne protein albumin, which carries GLP-1 around the body and protects it from enzymatic degradation and renal clearance. To avoid immunoreactivity, both molecules hew closely to the sequence of human GLP-1. Arginine (R) replaces lysine at position 34, leaving only one lysine (K), at position 26, that can react with glutamic acid or the linker, thus ensuring that attachment occurs at the right spot. In liraglutide (middle), glutamic acid connects the GLP-1 core to a fatty acid that contains 16 carbons; this drug is administered once a day. In semaglutide (bottom), alpha-aminoisobutyric acid (X) in semaglutide replaces alanine (A), which protects the molecule from destruction by the enzyme DPP-4, and a long, hydrophilic linker connects an 18-carbon di-acid to the GLP-1 moiety. Semaglutide is administered once a week as a subcutaneous injection. Illustration: Cassio Lynm / © Amino Creative
Semaglutide gained FDA approval for treating diabetes (Ozempic®) in 2017 and obesity (Wegovy®) in 2021. The agent fosters almost twice as much average weight loss as liraglutide does: 28 pounds over 16 months. Semaglutide’s side effects are mostly minor, but serious gastrointestinal problems cause some individuals to discontinue the drug. More than one million people in the U.S. have received prescriptions for Wegovy® since it entered the market.
Liraglutide and semaglutide have opened new avenues to powerful second-generation drugs. Eli Lilly’s tirzepatide, which contains not only GLP-1, but also another incretin called GIP, promotes even more dramatic effects than semaglutide does. The company has added glucagon to further fortify it, and individuals on a candidate called retatrutide lose, on average, more than 20% of their body weight.
Unlike GLP-1’s impact on diabetes, which maps primarily to the pancreas, its appetite-suppression activities lie mainly in the brain, and numerous investigators, including Knudsen, are detailing its behavior there. Researchers are probing its use in a tremendous range of illnesses, including chronic kidney disorders, fatty liver disease, neurodegenerative conditions such as Alzheimer and Parkinson’s diseases, and addiction. GLP-1-based therapies also protect the cardiovascular system, and earlier this year, the FDA approved semaglutide to reduce heart attack and stroke in people who have preexisting cardiovascular disease and are overweight or obese.
In addition to the scientists above, many others made key contributions to the GLP-1 story. These individuals include the late Werner Creutzfeldt (University of Göttingen), Richard DiMarchi (then at Eli Lilly), Daniel Drucker (University of Toronto), John Eng (then at the Bronx Veterans Affairs Medical Center), Jens Holst (University of Copenhagen), Michael Nauck (Ruhr-University Bochum), and Nancy Thornberry (then at Merck).
Through their ambitious and committed endeavors, Habener, Mojsov, and Knudsen have transformed the health prospects for the tremendous number of people whose surplus weight compromises their wellbeing. Their work has launched a new battery of blockbuster drugs that is propelling GLP-1 into a pharmaceutical realm with unprecedented reach.
by Evelyn Strauss
Selected Publications Joel F. Habener, Svetlana Mojsov, and Lotte Bjerre Knudsen
Lund PK, Goodman RH, Dee PC, and Habener JF. (1982). Pancreatic preproglucagon cDNA contains two glucagon-related coding sequences arranged in tandem. Proc. Natl. Acad. Sci. USA. 79, 345-349.
Mojsov S, Heinrich G, Wilson IB, Ravazzola M, Orci L, and Habener JF. (1986). Preproglucagon gene expression in pancreas and intestine diversifies at the level of post-translational processing. J. Biol. Chem. 261, 11880-11889.
Mojsov S, Weir GC, and Habener JF. (1987). Insulinotropin: glucagon-like peptide I (7-37) co-encoded in the glucagon gene is a potent stimulator of insulin release in the perfused rat pancreas. J. Clin. Invest. 79, 616-619.
Mojsov S. (1992). Structural requirements for biological activity of glucagon-like peptide-I. Int. J. Pept. Prot. Res. 40, 333-343.
Nathan DM, Screiber E, Fogel H, Mojsov S, and Habener JF. (1992). Insulinotropic actions of glucagon-like peptide-I (7-37) administered to diabetic and non-diabetic human subjects. Diabetes Care. 15, 270-276.
Knudsen LB, Nielsen PF, Huusfeldt PO, Johansen NL, Madsen K, Pedersen FZ, Thøgersen H, Wilken M, and Agersø M. (2000). Potent derivatives of glucagon-like peptide-1 with pharmacokinetic properties suitable for once daily administration. J. Med. Chem. 43, 1664-1669.
Madsen K, Knudsen LB, Agersoe H, Nielsen PF, Thøgersen H, Wilken M, Johansen NL. (2007). Structure-activity and protraction relationship of long-acting glucagon-like peptide-1 derivatives: importance of fatty acid length, polarity, and bulkiness. J. Med. Chem. 50, 6126-6132.
Knudsen LB, and Lau J. (2019). The discovery and development of liraglutide and semaglutide. Front. Endocrinol. 10, 1-32.

The boogie-woogie approach to creativity in art and science
The Dutch painter Piet Mondrian, famous for his geometric grid paintings, was an ardent jazz fan. In the late stage of his career, he became intrigued with boogie-woogie music, which inspired him to paint his masterpiece, Broadway Boogie Woogie.
Award Presentation: Richard Lifton
Obesity is a major public health problem affecting more than 40% of U.S. adults and 1 billion people worldwide. This is literally a growing problem; since 1960, average adult weight in the US has increased more than 30 pounds, attributed in part to reduced physical activity and ready availability of highly processed foods that are dense in calories.
Obesity has a significant impact on health and longevity. It is the major risk factor for type 2 diabetes, defined by chronic elevation in blood glucose levels; 90% of the 38 million type 2 diabetics in the US are overweight.
These considerations set the stage for today’s Lasker~Debakey Clinical Medical Research Award, as we recognize three scientists, Svetlana Mojsov, Joel Habener and Lotte Knudsen for their remarkable discoveries that have resulted in the development of revolutionary medicines that safely lower blood glucose in diabetics and induce profound weight loss that reduces obesity’s comorbidities.
The story starts 1906 with a report that an extract of intestinal tissue could lower blood glucose, but no progress was made toward purifying this factor. The story was revived in the 1960s when oral administration of glucose was found to produce a greater increase in insulin secretion than the same dose administered intravenously, suggesting that release of a gut hormone was priming the pancreas for insulin secretion in response to a meal. But the responsible factor, a so-called incretin, remained elusive.
The development of recombinant DNA technology in the 1970s provided new opportunities for gene discovery and connected the paths of two of today’s honorees. Svetlana Mojsov, as a graduate student with Bruce Merrifield at Rockefeller University, developed novel methods of solid phase peptide synthesis that enabled her to synthesize the short peptide hormone glucagon, which protects against hypoglycemia. In parallel, Joel Habener, an endocrinologist at MGH, cloned DNA copies of the messenger RNA encoding glucagon from the anglerfish. He found that the glucagon peptide was embedded in a longer precursor protein and snipped out by specific cuts. Surprisingly, he found that the precursor protein included another peptide sequence related to the glucagon family that was previously unidentified.
The following year, the homologous gene from hamster was cloned, and glucagon was again embedded in a larger precursor protein along with another potential peptide that was very similar to the anglerfish peptide; this peptide was named GLP-1.
As fate would have it, the hamster gene publication coincided with Svetlana Mojsov’s arrival on the faculty of MGH as director of the peptide synthesis facility. Svetlana dove into these publications with several critical questions- what was the active form of GLP-1, where was it produced, and what does it do? Svetlana’s experience led her to deduce that the active peptide would comprise 31 amino acids. She then used her skills to synthesize large quantities of the 31 amino acid peptide and made antibodies to it. She and Habener teamed up to show that the peptide was produced in the intestine; they published these results in 1986. It did not escape their attention that this peptide might be the long-sought incretin hormone.
To test this idea, Mojsov and Habener collaborated with Gordon Weir, showing that miniscule quantities of this peptide dramatically increased insulin secretion by the rat pancreas. Related findings were published by Holst in Copenhagen. Habener’s postdoc Daniel Drucker, Mojsov and Habener also showed that GLP-1 induced glucose-dependent insulin secretion from a pancreatic islet cell line. A story was emerging. Infusion of GLP-1 into healthy humans and diabetics by several groups established the role of GLP-1 as an incretin and a potential therapeutic for diabetes.
There was, however, a challenge: the half-life of GLP-1 in plasma was only 1-2 minutes. A much longer half-life would be essential. Enter Lotte Knudsen, a medicinal chemist at Novo Nordisk, determined to not just to develop a drug for diabetes, but to also determine whether GLP-1 might be another long-sought drug—one that safely and effectively causes weight loss. This speculation derived from the discovery by Stephen Bloom in London that injection of GLP-1 into the intracerebral ventricles strongly inhibited feeding in fasted rats. Thus began a saga that saw Knudsen’s teamwork for nearly 20 years to maximize the half-life of GLP-1.
In 2010 Novo Nordisk gained FDA approval for once-a-day subcutaneous injection of a modified form of GLP-1, liraglutide. Liraglutide also produced ~5 lb. weight loss, giving Knudsen and her team the encouragement to press on. Over the next 5 years, after testing thousands of modifications, the team reported the development of semaglutide, a highly modified GLP-1. Semaglutide was strong enough binding to albumin in plasma to prevent its degradation and filtration by the kidney while preserving robust activation of its pancreatic receptors to stimulate insulin secretion. This chemical tour de force increased semaglutides half-life two thousand fold, allowing once-weekly subcutaneous injection. In 2017, semaglutide received FDA approval for treatment of diabetes at a dose of 1 mg. per week.
But the biggest surprise came when the dose was increased from 1 mg to 2.4 mg per week: not only was blood glucose control excellent, but weight loss was astounding – obese people without diabetes lost on average 15% of their starting weight (more than 30 pounds in a person starting at 220 pounds). This led to FDA approval of high dose semaglutide for weight loss in 2021.
This weight reduction was not merely cosmetic. Placebo- controlled trials of semaglutide in people with existing cardiovascular disease reduced CV death, heart attack or stroke by 20%. Similarly, In diabetics with progressive kidney failure, treatment significantly reduced progression and the need for dialysis or kidney transplantation. Promising results have also been seen in obesity-related fatty liver with fibrosis. Recently, a real-world observational study comparing GLP-1s to insulin for diabetes showed that GLP-1s reduced the incidence of 10 different obesity-related cancers by 25% to 65%. GLP-1s are also being tested in diseases ranging from Parkinson’s disease to a range of compulsive or addictive behaviors. Better understanding of GLP-1’s mechanism of action and how to best sustain weight loss are matters of intense investigation.
Word of these dramatic results spread like wildfire, and uptake of GLP-1s has been meteoric. Semaglutide has been taken by literally millions of people in the US in the last three years.
To no one’s surprise, the rest of the biotech and pharmaceutical industry has noticed. Eli Lilly has developed tirzepatide, which adds activity of another incretin-like peptide, GIP, to the GLP-1 backbone. Tirzepatide produced a 21% average weight reduction in non-diabetics and was FDA approved for weight loss in 2023. Oral versions of GLP-1s have also been approved, though they thus far have lower efficacy.
It is hard to overestimate the potential of these remarkable discoveries for human health. In their 1968 recording of Revolution #1 the Beatles’ John Lennon sang, “You say you want a revolution, well you know, we all want to change the world.” GLP-1s and their successors are well on the road to changing the world, and Svetlana Mojsov, Joel Habener and Lotte Knudsen are recognized today as the revolutionaries who lit the match. Congratulations to this year’s recipients of the Lasker~DeBakey Clinical Medical Research Award.
Acceptance remarks
Acceptance Remarks: Joel Habener
As I look back on my nearly 60 years of biomedical research, I realize how important serendipity was in shaping of my career in research.
My first unanticipated serendipitous event occurred in 1967 when, because of the outbreak of the Vietnam war, I was drafted into the US Public Health Service and assigned to the NIH to undertake two years of laboratory research on the mechanisms of DNA replication. While I was at the NIH, the first studies were just beginning that inaugurated the field of molecular biology. My experience at the NIH was a tremendous inspiration.
The next serendipitous event occurred while I was at the NIH when I met John Potts, who invited me to join his staff in his newly-appointed position as the chief of the endocrine unit at the MGH. I obtained a Special NIH Fellowship to study the processes of the biosynthesis of parathyroid hormone. However, a problem arose–the Endocrine Unit was not yet equipped to conduct the studies.
Again, purely by chance, serendipity intervened. I was introduced by a mutual friend to Alexander Rich, a molecular biologist at MIT, who invited me to join his lab and to work collaboratively with John Potts and a post-doc, Byron Kemper. Our studies led to my appointment as an investigator in the Howard Hughes Medical Institute, which supported my work at the MGH for 30 years.
With the support of the HHMI, I decided to investigate the causations of type 2 diabetes, a disorder of insulin resistance. My newly-recruited post-docs Kay Lund and Dick Goodman and I planned to use recombinant DNA technology to clone the gene for glucagon using the hormone-producing islets isolated from the rat pancreas. But our plans were upset by a moratorium on recombinant DNA studies in warm-blooded animals. Again, serendipity intervened. We learned that fish, cold-blooded animals, make their pancreatic hormones in an organ that is separate from the exocrine pancreas (Brockmann bodies), thus greatly facilitating the preparation of high-quality messenger RNA to prepare the cDNA for cloning. The use of the Anglerfish Brockmann bodies greatly facilitated our work that identified the fish homolog of GLP-1.
Acceptance Remarks: Lotte Bjerre Knudsen
I am truly honored to receive this award, and I want to offer my profound gratitude to the Lasker Foundation and the jury for including me. The Lasker Foundation celebrates scientific and medical advances, and that is very important. The story of GLP-1 fits perfectly within this.
Science is rarely a solitary endeavor. Great scientific breakthroughs demand perseverance, a willingness to embrace risk, and to work effectively and selflessly with others. In accepting this award, I do so on behalf of countless brilliant individuals who have been part of this journey.
Most of my scientific journey has unfolded over 35 incredible years at Novo Nordisk. I was responsible for the invention of the first long-acting GLP-1, and proposed we should focus on obesity as well as diabetes. At the time, the notion that one molecule could have two separate effects was provocative, as was the thought of having a novel injectable medicine for these conditions. I passionately believed in the molecule and its potential for both diseases, and I have continued to be a part of the unfolding scientific narrative surrounding GLP-1 over those 35 years.
This award gives me a chance to highlight the work we do in the pharmaceutical industry. The case of GLP-1 illustrates how numerous inventions were needed before we arrived at a medicine that induces double-digit per cent weight loss as well as reduced cardiovascular disease risk in obesity. Aside from the inventions, countless people did and still do important work to generate the clinical evidence required, and to get these medicines to the people who need them. Especially when it comes to developing medicines for obesity; I have spent more than three decades in a company that encouraged scientific discoveries in several diseases, including diabetes and obesity, and progressed them at a time when few companies believed in medical treatment for obesity, or indeed in GLP-1.
Outside the pharmaceutical industry, many leaders in medicine continue to advocate for obesity as a serious chronic disease, and for access to evidence-based treatments to reduce the burden patients face, much work still needs to be done, and these medicines may serve as a catalyst in the dialogue.
Breakthrough discoveries require vision as well as courage. By their very nature, they only materialize at the end of a long process—when odds, obstacles and objections have been overcome. My message to all aspiring young scientists is to believe in your ideas and pursue them with determination. Never be afraid to suggest something novel. A life where scientific thinking guides you is always a truly exciting one.
Acceptance Remarks: Svetlana Mojsov
I am very honored to receive the Lasker~DeBakey Clinical Medical Research Award for my contribution to the discovery of GLP-1.
Forty-one years ago, on November 4, 1983, I began to synthesize GLP-1 peptides by the solid phase method in my Laboratory at the Endocrine Unit in the Bulfinch Building in Massachusetts General Hospital in Boston. All my syntheses were done on a manual shaker invented by my PhD mentor Bruce Merrifield in the 1960s, when he developed the solid phase method for the synthesis of peptides and proteins that forever changed the field of peptide chemistry. In 1983, manual shakers were not available commercially. They were made by the Instrument Shop at the Rockefeller University and Dr. Merrifield sent me one from his laboratory.
That was the beginning of a scientific journey that involved collaborations between large number of chemists with biologists and clinicians—first in academia, and later in pharmaceutical companies. Our joint efforts led to the development of GLP-1 analogs for diabetes and obesity.
It is my privilege to have been there at the very beginning.
Thank you very, very much.
