
H. Michael Shepard
Genentech

Dennis J. Slamon
University of California, Los Angeles

Axel Ullrich
Max Planck Institute of Biochemistry
For their invention of Herceptin, the first monoclonal antibody that blocks a cancer-causing protein, and for its development as a life-saving therapy for women with breast cancer
The 2019 Lasker~DeBakey Clinical Medical Research Award honors three scientists—H. Michael Shepard, Dennis J. Slamon, and Axel Ullrich —who invented Herceptin, the first monoclonal antibody that blocks a cancer-causing protein, and developed it into a life-saving therapy for women with breast cancer. The innovation reduces the risk of recurrence and extends survival time for patients with metastatic as well as early-stage disease. Every year, more than 50,000 women in the US are diagnosed with the type of breast cancer that the drug attacks, and over 2.3 million individuals have received the treatment since it became available. Shepard (now at BetterOutcomes4Cancer) and Ullrich (now at Max Planck Institute of Biochemistry, Martinsried, Germany) conducted their Herceptin investigations at Genentech. Slamon did his at the University of California, Los Angeles (UCLA), where he continues to work.
In the mid 1970s, scientists discovered that genes within our own bodies can trigger cancer. This revelation sparked the idea that stifling the activities of such oncogenes might thwart the trouble they instigate. This approach—in which a therapy would fixate on molecules that dwell specifically in cancer cells and also drive malignancy—held great appeal. Such a targeted strategy might avoid many of the harsh side effects associated with chemotherapy while striking the source of the affliction.
They saw HER standing there
Prominent among known oncogenes were several that encode overzealous versions of growth factors and the receptors that sense them. The receptors, which lie across the cell membrane, receive signals from the external environment and then relay them inside to spur proliferation. Ullrich was particularly interested in a subgroup of these proteins—the tyrosine kinase receptors—and he wanted to uncover previously unknown members of this molecular family in humans.
In 1985, Ullrich, Arthur Levinson (also at Genentech), and colleagues found a gene whose sequence resembles that of the human epidermal growth factor receptor (EGFR or HER1) and the chicken oncogene v-erbB. They named it HER2—human EGF receptor 2—because of this similarity. Its sequence and location on the chromosome suggested that it might be the human version of neu, a rat oncogene discovered the year before by Robert Weinberg (Massachusetts Institute of Technology). Independently and simultaneously, two other groups, led by Stuart Aaronson (National Cancer Institute) and Tadashi Yamamoto (University of Tokyo), identified HER2 and showed that it was amplified in malignancies from a human breast and a salivary gland.
In the meantime, UCLA oncologist Slamon and, independently, the late William McGuire (University of Texas Medical Center, San Antonio), had been collecting cancer tissues that had been surgically removed for therapeutic reasons and checking whether established oncogenes were firing excessively in them. Ullrich, with his tantalizing gene, and Slamon, with his human tumor library, connected. In 1987, they reported that almost 30% of 189 breast cancer samples contained more than one copy of the HER2 gene. Analysis of health records for many of the patients represented in the study revealed that women whose tumors carried multiple copies of the gene relapsed more quickly and died sooner than did those whose tumors contained only one copy. Furthermore, the gene amplification better predicted prognosis than did most standard indicators, such as tumor size and hormone receptor status.
These associations were provocative, but numerous previously described proteins appeared on cancer cells yet did not propel tumor formation or progression. To gain candidacy as a therapeutic target, HER2 overabundance would have to cause, not just correlate with, malignancy.
To investigate this issue, Ullrich and postdoctoral fellow Robert Hudziak engineered mouse connective-tissue cells grown in laboratory culture dishes to produce extra HER2 protein. The supplemental HER2 caused the cells to keep dividing under conditions in which they’d usually stop, a sign of transformation to a cancerous state. The HER2-augmented cells also displayed other evidence of malignancy, and they formed tumors after injection into mice. Because the only difference between the corrupt and well-mannered cells was the amount of HER2, these results indicated that surplus growth factor receptor unbridles normal restraints on replication.
Simultaneously and in parallel, Shepard, in his own lab at Genentech, had landed on HER2 from a different direction. He was probing the mechanisms by which cancer cells evade destruction by a chemical called Tumor Necrosis Factor-α (TNF-α), a component of the body’s immune response. He had found that activation of some tyrosine kinases can curb TNF-α’s lethal potency. Together, he and Ullrich showed that HER2 renders mouse cells resistant to TNF-α’s toxic effects. Perhaps, they reasoned, HER2 promotes aggressive cancers not only by causing growth to run amok, but also by toughening up the cells and endowing them with ways to withstand assaults that normally would kill them.
If excessive quantities of HER2 cause runaway growth and protection from the body’s defense system, quashing receptor function might reverse these aberrant behaviors. The part of the protein that resides outside the cell was especially alluring because it was likely to be accessible to a drug. To block HER2 stimulation, the researchers wanted to develop a compound that would bind to this exposed portion and impede incoming signals. They sought monoclonal antibodies to serve that purpose.
HER promise revealed
The Genentech scientists made a collection of monoclonal antibodies in mice and zeroed in on one that inhibited growth of several breast cancer cell lines. Crucially, it had this effect only on cell lines that overproduce HER2 protein. Furthermore, it sensitized these tumor cells to killing by TNF-α. The top pick antibody, dubbed 4D5, did not bind to HER2’s relative, the human EGF receptor—an important characteristic, as a successful drug must not interfere with activities of healthy cells. These observations suggested that a 4D5-based treatment would foil only HER2-overexpressing cells.
Even if 4D5 could, in principle, crush tumor growth in people’s bodies, a significant hurdle remained. Because it came from mice, the human immune system would deem it “foreign” and destroy it. To design an antibody that would not stir such an inflammatory reaction, Paul Carter, working with Shepard, aimed to retain the bare minimum of 4D5—only the part that binds HER2—and replace the rest with human antibody sequences. In 1992, the team reported that one of these “humanized” antibodies bound HER2 three times more tightly than 4D5 and blocked proliferation of a HER2-overexpressing breast cancer cell line as efficiently.
Despite these auspicious results, hesitation lurked among Genentech’s decision makers. The company had pursued other potential cancer drugs that had not panned out. Furthermore, many experts were skeptical that monoclonal antibodies would prove therapeutically useful against cancer, especially for solid rather than blood malignancies—in part because scientists doubted that these agents would penetrate the tumors. To bolster the case for clinical pursuit, Shepard and Slamon performed numerous studies. They showed, for instance, that radioactive-tagged mouse antibody—a single dose, so it would not elicit a strong immune response—accumulated in tumors, but only in those of women with cancers that overproduced HER2. This encouraging observation energized the team, as did the patients’ willingness to participate even though they would not benefit and might suffer unknown consequences. Such generosity repeated itself at numerous steps of the enterprise.
During this period, the investigators also collected data that would help guide clinical deployment of the potential drug. Using human breast cancer cells grown in the lab, Slamon and colleagues explored how best to combine the antibody with standard chemotherapy regimens. Genentech scientists and Slamon also developed diagnostic tests to identify women with HER2-overexpressing (HER2+) breast cancers.
Troublemaker transformed into target
The company decided to move forward, and clinical trials began on women with metastatic HER2+ breast cancer. By 1998, the data were strong enough that the humanized monoclonal antibody—now called trastuzumab (brand name, Herceptin)—gained approval by the U.S. Food and Drug Administration (FDA).
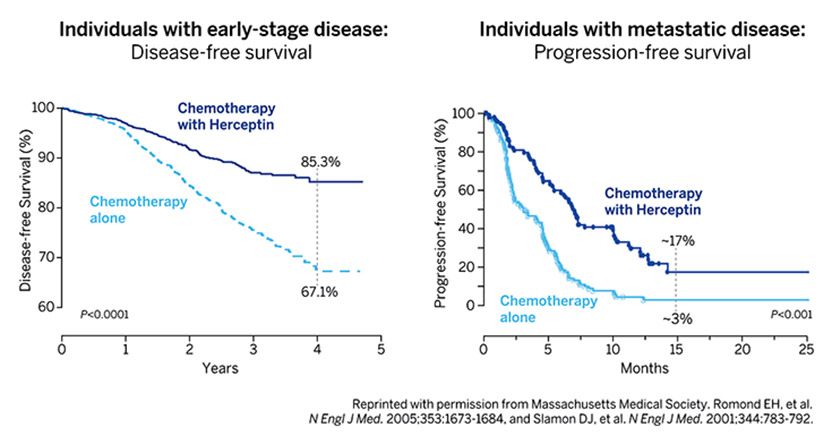
In 2001, Slamon and colleagues published those results. A large, randomized study on women with progressive, HER2+ breast cancer revealed that the addition of Herceptin to chemotherapy stalled disease progression, reduced the one-year death rate from 33 percent to 22 percent, and extended overall survival. Subsequent trials on early-stage, HER2+ breast cancer showed that Herceptin also improves outcomes in that setting, for which it was FDA-approved in 2006 (see Figure).
Beating back breast cancer
Women with early-stage (left) or metastatic (right) HER2+ breast cancer were treated with either Herceptin plus chemotherapy or chemotherapy alone. The percentage of women with early-stage breast cancer who were alive and free of disease four years after beginning the trial was significantly higher if they received Herceptin (85.3 %) than if they did not (67.1 %). The percentage of women whose metastatic disease had not progressed 15 months after beginning the trial was significantly higher if they received Herceptin (~17.5%) than if they did not (~3%).
Herceptin is now a standard therapy for HER2+ breast cancers. Researchers have continued to investigate HER2, and additional antibodies that target it have reached the market. For instance, a drug called pertuzumab differs from Herceptin in the region of HER2 that it binds and its mechanism of action. A 2015 review reported that overall survival of women with metastatic HER2+ disease who received chemotherapy plus pertuzumab and Herceptin was more than 4.5 years. In 2001, life expectancy for women with that diagnosis was 1.5 years.
The impact of Herceptin’s development reaches beyond breast cancer by establishing that monoclonal antibodies can indeed combat solid tumors. Furthermore, the innovation offers a new model for personalized medicine by deploying a diagnostic test that identifies the most appropriate patients to treat with a particular intervention. By uncovering and exploiting the molecular pathology of a devastating disease, Shepard, Slamon, and Ullrich conceived and executed a new blueprint for drug discovery that has already bestowed tens of thousands of women with time and quality of life.
by Evelyn Strauss
Key Publications on Herceptin – Its Invention and Clinical Development
Coussens, L., Yang-Feng, T.L., Liao, Y.-C., Chen, E., Gray, A., McGrath, J., Seeburg, P.H., Libermann, T.A., Schlessinger J., Francke, U., Levinson, A., and Ullrich, A. (1985). Tyrosine kinase receptor with extensive homology to EGF receptor shares chromosomal location with neu oncogene. Science. 230, 1132-1139.
Hudziak, R.M., Schlessinger, J., and Ullrich, A. (1987). Increased expression of the putative growth factor receptor p185-HER2 causes transformation and tumorigenesis in NIH 3T3 cells. Proc. Natl. Acad. Sci. 84, 7159-7163.
Slamon, D.J., Clark, G.M., Wong, S.G., Levin, W.J., Ullrich, A., and McGuire, W.L. (1987). Human breast cancer: correlation of relapse and survival with amplification of the HER2 protooncogene. Science. 235, 177-182.
Hudziak, R.M., Lewis, G.D., Shalaby, M.R., Eessalu, T.E., Aggarwal, B.B., Ullrich, A., and Shepard, H.M. (1988). Amplified expression of the HER2/ERBB2 oncogene induces resistance to tumor necrosis factor-alpha in NIH 3T3 cells. Proc. Natl. Acad. Sci. USA. 85, 5102-5106.
Slamon, D.J., Godolphin, W., Jones, L.A., Holt, J.A., Wong, S.G., Keith, D.E., Levin, W.J., Stuart, S.G., Udove, J., Ullrich, A., and Press, M.F. (1989). Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science, 244, 707-712.
Hudziak, R.M., Lewis, G.D., Winget, M., Fendly, B.M., Shepard, H.M., and Ullrich, A. (1989). p185HER2 Monoclonal antibody has antiproliferative effects in vitro and sensitizes human breast tumor cells to tumor necrosis factor. Mol. Cell. Biol. 9, 1165-1172.
Shepard, H.M., Lewis, G.D., Sarup, J.C., Fendly, B.M., Maneval, D., Mordenti, J., Figari, I., Kotts, C.F., Palladino, Jr., M.A., Ullrich, A., and Slamon, D. (1991). Monoclonal antibody therapy of human cancer: taking the HER2 protooncogene to the clinic. J. Clin. Immunol. 11, 117-127.
Carter, P., Presta, L., Gorman, C.M., Ridgeway, J.B., Henner, D., Wong, W.L., Rowland, A.M., Kotts, C., Carver, M.E., and Shepard, H.M. (1992). Humanization of an anti-p185HER2 antibody for human cancer therapy. Proc. Natl. Acad. Sci. USA. 89, 4285-4289.
Pegram, M.D., Lipton, A., Hayes, D.F., Weber, B.L., Baselga, J.M., Tripathy, D., Baly, D., Baughman, S.A., Twaddell, T., Glaspy, J.A., and Slamon, D.J. (1998). Phase II study of receptor-enhanced chemosensitivity using recombinant humanized anti-p185 HER2/neu monoclonal antibody plus cisplatin in patients with HER2/neu-overexpressing metastatic breast cancer refractory to chemotherapy treatment. J. Clin. Oncol. 16, 2659-2671.
Slamon, D.J., Leyland-Jones, B., Shak, S., Fuchs, H., Paton, V., Bajamonde, A., Fleming, T., Eiermann, W., Woldter, J., Pegram, M., Baselga, J., and Norton, L. (2001). Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 344, 783-792.
Shepard, H.M., Jin, P., Slamon, D.J., Pirot, Z., and Maneval, D.C. (2008). Herceptin. In Therapeutic Antibodies. Handbook of Experimental Pharmacology. Edited by Y. Chernajovsky and A. Nissim, Springer-Verlag, Berlin, Heidelberg. pp. 183-219.

Seurat’s Dots: A Shot Heard ‘Round the Art World
How the color theories of a chemist have ricocheted across centuries of artistic and scientific imagination.
Award presentation by Michael Brown
Each year 250,000 American women are diagnosed with breast cancer. Twenty percent are caused by extra copies of a gene called HER2. Until recently the 50,000 women with HER2-positive breast cancer had a terrible prognosis. Today the finding of HER2 is good news. When a breast biopsy is HER2 positive and the cancer has not advanced beyond regional lymph nodes, that woman has a 90% chance of being tumor-free for at least 3 years and likely forever. These cures come from an antibody called Herceptin that targets HER2. When Herceptin was approved in 1998 it was the first monoclonal antibody against an oncogene. This single drug changed our entire approach to cancer therapy. It emerged from the work of 3 scientists: Axel Ullrich and Michael Shepard of Genentech, and Dennis Slamon of UCLA.
A Lasker Award for cancer is appropriate because the invention of Herceptin can be traced to our patron saint Mary Lasker. Throughout the 1960’s Mary stalked the lobbies of Congress and the White House advocating fiercely for cancer research. Her lobbying bore fruit in 1971 when President Nixon launched the War on Cancer, and Congress appropriated 1.6 billion 1971 dollars.
Acceptance remarks
Acceptance remarks, 2019 Lasker Awards Ceremony
To be recognized by a Lasker award is amazing. To have this recognition together with the other awardees, like Dennis and Axel, is humbling. To have had a part in such an innovative project, which has done so much good for so many people, is a bit overwhelming. More than 2 million patients have been treated, many of whom have benefited tremendously. Herceptin is a breakthrough drug and led the way for other highly targeted therapies. Just the same, even though it has done much good and changed many lives for the better, it is not perfect. As a scientist deeply committed to this kind of work, I often remind myself, involuntarily, that although as many as 15% of breast cancer patients are helped by Herceptin, the majority are not. There remains a lot to be done, and I think that those of us who have suceeded to the extent we have done, must now be deeply involved with the next generations of scientists and clinicians who will carry this work forward. There is a lot of mentoring to do. Among other things, we must teach that having really big goals, being a dreamer, is a good thing. Young people must believe that. Perhaps right now more than in other times.
The Herceptin project evolved from an idea to create a safe cancer therapeutic. Many have come before us, and hopefully others will follow. We all had to overcome scientific difficulties…and myths. One of the most interesting myths for Herceptin was that monoclonal antibodies could not penetrate solid tumors. Luckily, the rigorous scientific environment of Genentech allowed us to directly address this issue and overcome it. We learned many other things during the course of this work, among them that the aggressiveness of HER2 tumors is in part due to creating tumor cell resistance to immune surveillance. Gail Phillips, who is here today, discovered that once tumor cells become resistant to macrophage killing, they can be subsequently stimulated by these immune cells. This is an example of how tumor cells can actually pervert antitumor responses to their benefit. Another thing that we learned during the whole process of creating Herceptin is that collaborations and communications between scientists, whether academic or biotech, drives breakthrough drug discovery and development.
Finally, it is difficult to see how I came to this place. The only explanation I can offer is that there were people along the way who believed in me, sometimes more than I believed in myself. Some of these people are here today, including George Malacinksi, my PhD mentor, and Marc Feldmann, with whom I have shared many years of scientific discussions and fellowship. I would like to thank them and all of my colleagues.
Acceptance remarks, 2019 Lasker Awards Ceremony
When Axel Ullrich, Mike Shepard and I first began the research journey that brought us here today, sharing this incredible honor, we actually shared very little else. However, what we did have in common was the intense curiosity that drives scientists to address questions of interest to them. Axel had an intense desire to identify, clone, characterize and understand the function of genes regulating cell growth. Mike was very interested in understanding how some cancers respond to innate host immunity mechanisms while others are resistant. My interests centered around two questions; first, why was there such diversity in outcomes for patients who supposedly had the same disease, i.e. lung cancer or colorectal cancer or breast cancer when treated with the “one-size-fits-all” therapies then used for malignancies arising in a given organ site; and second, what role if any did the new class of genes known as “oncogenes” play in these diseases.
Clichés frequently exist because they represent truth. That is clearly true with the saying, “those who accomplish something frequently stand on the shoulders of others.” In my case, that is a gross understatement. Each of us owe much of what we are being honored for today to what we learned from the work of others. I was heavily influenced by a mentor, Janet Rowley, who taught me that recurrent changes seen in the DNA of many malignancies are not just random noise secondary to instability of cancer genomes but can yield important information about the genesis and behavior of the diseases in which they occur. In Werner Kirsten’s lab, I worked with the Kirsten sarcoma virus, an acutely transforming retrovirus which was later shown to owe its profound cancer-inducing phenotype to carrying the K-ras oncogene. Indeed, I first learned about the whole class of “oncogenes” and the fact that they are really altered derivatives of genes that regulate normal cell growth from the work of two prior awardees, Mike Bishop and Harold Varmus.
Armed with this background, I began probing DNA, RNA and proteins from various human cancer tissues removed therapeutically, looking for alterations in these genes and publishing our first results in 1984. This initial work led to the pivotal 1986 collaboration with Axel Ullrich who had identified six growth-related genes, including HER2. We were agnostic in our initial approach to studying these genes and evaluated a large series of different cancers for changes in them without much success until we came to breast cancer tissues. It was here we first saw that HER2 was amplified in about 20-25% of the cases and developed the initial evidence that HER2 amplification identified a new subtype of breast cancer; those with the worst outcomes despite being treated using our best available standard therapies. By then, Bob Weinberg had shown that the murine counterpart of HER2, when mutated, would cause brain malignancies in rats and Jeff Drebin subsequently demonstrated that antibodies directed against the protein made by this mutated murine-HER2 version would inhibit growth of mouse tumors. Again learning from colleagues, Mike and Axel at Genentech and we at UCLA undertook preclinical testing of a series of HER2 antibodies and saw similar growth inhibition of HER2-driven cell lines and experimental tumors. This preclinical work culminated in the subsequent clinical development and eventual approval of the drug Herceptin that has now changed the natural history of patients with HER2-positive breast cancer from those with the worst outcomes to those with the best.
Finally, the three of us and more than 3 million women globally, also stand on the shoulders of a small group of women who volunteered to participate in the initial clinical trials ultimately resulting in approval of Herceptin. They are not research subjects or study numbers but are also colleagues in every sense of the word. We owe them a profound gratitude as well. The lessons learned on all these shoulders; those of colleagues and patients, as well as the platforms we initially built to study HER2, continue to inform us today and recently led to research resulting in approval of agents targeting the cdk-4 and 6 kinases and producing major outcome improvements for hormone receptor-positive breast cancer, the largest subtype of this disease.
I have had the empowering advantage of standing on the shoulders of others including my co-awardees and I thank all of those many individuals and you for this amazing honor.
Acceptance remarks, 2019 Lasker Awards Ceremony
More than a hundred years ago, Paul Ehrlich, the founder of chemotherapy, received the Nobel Prize for Physiology or Medicine. He postulated ‘man muß zielen lernen, chemisch zielen lernen’ (you have to learn targeting, chemically targeting) – to find ‘magic bullets’ – chemical substances that might have special affinities for cancer cells in the fight against human diseases. This concept inspired generations of scientists, including me.
Since I was a boy, I had developed an interest in everything that lived – plants and animals. After studying biochemistry in Tübingen, I went on to do my PhD in Heidelberg. I was always interested in the application of science and I wanted to do something medically important. I had read about the newly emerging gene technologies in the mid-seventies and was very excited. UCSF was a cosmos of creativity. I started to work on insulin, on cloning insulin cDNA, and I succeeded. From then on, my research and my career developed along a path that really started with basic scientific curiosity, but in a field that was very close to application. That my work led to cancer research was not planned either. This came out of my interest in growth factors and their receptors, and suddenly there was this connection to cancer. The discovery of HER2/neu, it’s role in breast cancer and the development of Herceptin – ‘the magic bullet’ – all resulted from that interest. However, as is common since long, all this work was a great team effort.
At the time of oncogene discoveries and in the early years of targeted therapy I was optimistic that cancer will be curable one day. I think you have to be a little bit naive to tackle large problems such as cancer. Today, I am more realistic – there is still a long way to cure cancer.
To receive the Lasker award is a great honor. I feel very grateful that so many patients with cancer have benefitted from our work – this is a dream come true for a scientist.
